Hypothermia Prevention, Detection and First Aid
Hypothermia in Open Water Swimming
by Nick Olmos-Lau M.D.
Temperature regulation is one of the most important functions in the preservation of normal biological
processes. The internal milieu of the organism is regulated by a process called homeostasis which functions optimally within a
very narrow range of temperatures. The internal temperature of a normal resting adult is around 37 C. The internal temperature
recorded from the rectum or the external auditory canal is less variable and more dependable than when the temperature is
registered orally or in the axilla, and is usually lower around 36.5C (98.6F).
When the temperature rises above 37.5 C (99F) fever occurs. This is usually one of the first line body's defenses against infection.
Hypothermia occurs when the body's temperature drops below 35C (95F). In both cases the function and metabolism of the various
body organs is altered.
 The generation of heat is closely linked to the production of energy. The production and elimination of heat are extremely precise
functions, controlled by complex metabolic-endocrine systems monitored by the Central Nervous System. These thermoregulatory
centers are located in the brain in the area of the hypothalamus.
The generation of heat is closely linked to the production of energy. The production and elimination of heat are extremely precise
functions, controlled by complex metabolic-endocrine systems monitored by the Central Nervous System. These thermoregulatory
centers are located in the brain in the area of the hypothalamus.
When the body loses heat at a greater speed than it can generate, a negative deficit develops with a net heat loss. The body
counteracts this negative deficit by development of chills. These are continuous inadvertent muscular contractions that generate
heat.
The body maintains its normal (euthermic) level utilizing several mechanisms to hold an even state. These mechanisms utilize
heat radiation, breathing, evaporation or sweat, convection (heat loss activated by wind), and conduction by proximity with other
objects. These mechanisms permit the body to shed excessive amounts of heat generated by high internal production such as with
heavy exercise or fever. For example during Marathon running race the body generates tremendous amounts of heat that it must
dispose of. However losing excessive amounts of heat could cause a hypothermic condition after running.
Biological processes and organs functions appear to cease when that internal temperature reaches approximately 26 C (80F).
Nevertheless, such temperatures are used during controlled medical procedures such as cardiac or brain surgery because there
is an element of reversibility. The opposite is not usually the case; temperatures over 43 C (108 F) can cause irreversible brain
damage.
Among the types of hypothermia described, land hypothermia is perhaps the most common. This occurs as a result of exposure to
cold, wind, rain, snow or freezing precipitation and is usually seen during high risk recreational or sports activities such as
mountaineering, climbing, skiing, prolonged exposure during hiking or snowmobiling.
Aquatic hypothermia occurs mainly during prolonged open water swimming, wind surfing, waterskiing, kayaking or boating when
sudden and persistent temperature drops occur, or with accidental falls in the water.
The first symptoms observed during land hypothermia are fatigue or tiredness associated with an intense desire to stop all activity or
movement. The person eventually collapses or faints. In such cases it is important to place the victim in a horizontal position,
remove their wet clothes, and try to maintain consciousness. If the person is awake warm drinks will help. Avoid tea, coffee or
alcohol as they may worsen the condition, because they worsen dehydration due to diuretic effects. When a person is already
unconscious one must not attempt to force fluids by mouth, as it could lead to fluid aspiration into the lungs. This is due the lack
of protective reflexes such as cough and an improper ability to swallow.
 Water immersion creates a higher risk for serious problems, because in the water the body can lose approximately 20 to 30 times
more heat than at the same temperature in land. This is due to the fact that the water which surrounds the body acts like a sponge
pulling out heat by the mechanism of conduction. When the internal temperature reaches 32 C (89.6 F), consciousness is usually lost
and can this can lead to drowning. Cardiac arrest (heart stoppage) and cardiac arrhythmias occur when the temperature of the
body reaches 30 C (86 F).
Water immersion creates a higher risk for serious problems, because in the water the body can lose approximately 20 to 30 times
more heat than at the same temperature in land. This is due to the fact that the water which surrounds the body acts like a sponge
pulling out heat by the mechanism of conduction. When the internal temperature reaches 32 C (89.6 F), consciousness is usually lost
and can this can lead to drowning. Cardiac arrest (heart stoppage) and cardiac arrhythmias occur when the temperature of the
body reaches 30 C (86 F).
Common advice to capsizing boat accident victims in cold waters, it is to hold onto their clothes, adopt a crouched position with their
arms crossed in front and keep floating. When there is a group of people it is recommended to hug each other to conserve and acquire
heat. Floating is preferable to swimming, when the person is further than a thousand yards from land because activity in cold water
will speed heat loss and promote hypothermia (except when the person is expert or adapted to cold water swimming). See figures
1 and 2. Immersion in water temperatures below 10 C (50 F) is of great danger, because severe hypothermia will develop in most
people in less than an hour.
Table No. 1 describes physiological changes observed in a person as the body temperature falls. It helps to create a mental
picture of a gradually worsening process, and offers suggested actions.
Table #1 |
Internal Temperature |
Symptom |
Action |
37.0C 98.6F |
Normal |
None |
36.0 |
Cold sensation with numbness of hands and feet |
Look for shelter. Take off wet clothes. External heat. Warm drinks |
35.0 |
Chills and tremors. Slurred speech |
As above |
<35C 95F |
|
Hospitalization |
34C 93.2F |
Irrational thoughts, Confusion, Incoordination, Memory problems |
Administer warm sweet drinks, Warm air rebreather, BP and Pulse check for
irregularities, Rest with leg elevation |
33C 91.4F |
Muscle rigidity |
|
32C |
Chills subside Collapse |
Transport to hospital as EMERGENCY |
30-31C 86F |
Loss of consciousness, Absence of pain reactions |
Protect airway |
29C 84.2F |
Slow Pulse, Low BP |
Prepare to start CPR |
28C 82.4F |
Cardio Pulmonary Arrest CPR, Absent Pulse and pupil Light reaction |
Chest compression |
<28C 80.6F |
Absent vital signs, Pulmonary edema |
Maintain CPR efforts until body is rewarmed to normal temp |
Survival after immersion in waters close to freezing temperature is extremely limited. Experts on this subject state that a person
immersed in the water, unprotected by adequate gear is likely to survive at the most six to seven minutes (C. Wennerberg). The
chances of survival are better, if the person is young and has a thick fat pad that can act as an insulating coating.
Case reports of boat accidents and plane crashes into waters with temperatures close to freezing conditions (WWII and the Korean
conflict) documented only one case only of verifiable survival. This was one marine of 10 that were shipwrecked near the
Aleutian Islands. The person who survived was recovered after a half-hour immersion in temperatures of 6-8 C (44-46F).
There was another case described of a 22-year-old airplane pilot who survived two hours of immersion in temperatures of 8-10
C (49-50F) in waters off Oregon State beaches.
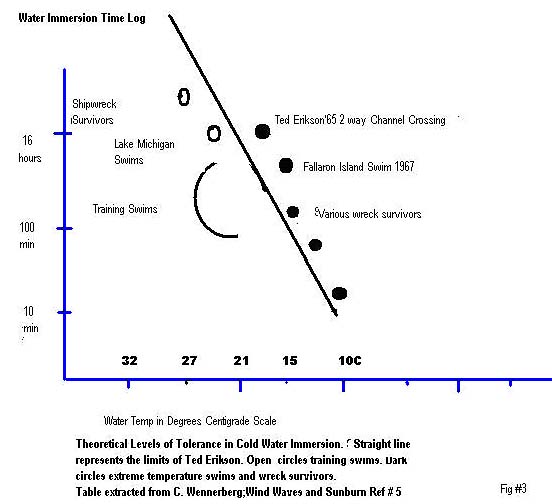 Figure #3 documents observations made in swimmers at various temperatures and conditions reported by Conrad Wennenberg in
his book Winds, Waves and Sunburn in 1997(Ref#5 A history of Marathon Swimming). In this book Wennerberg describes long
swims performed by outstanding swimmers, and compares them with the documented survivals after prolonged exposure in cold
water. He was able to establish a linear relation between length of immersion and water temperatures. An extrapolation of his
calculations would indicate that a swimmer could remain safely for indefinite periods in water temperatures of 95-98F (35-37F).
However survival would be seriously compromised after a 16 hour exposure in water at 15-17 C (59-62F).
Figure #3 documents observations made in swimmers at various temperatures and conditions reported by Conrad Wennenberg in
his book Winds, Waves and Sunburn in 1997(Ref#5 A history of Marathon Swimming). In this book Wennerberg describes long
swims performed by outstanding swimmers, and compares them with the documented survivals after prolonged exposure in cold
water. He was able to establish a linear relation between length of immersion and water temperatures. An extrapolation of his
calculations would indicate that a swimmer could remain safely for indefinite periods in water temperatures of 95-98F (35-37F).
However survival would be seriously compromised after a 16 hour exposure in water at 15-17 C (59-62F).
He was able to also demonstrate and document the capacity of adaptation of human beings through training. Adaptation and
training could increase tolerance and lengthen the time of exposure to these challenging conditions.
Our limitations however, are quite evident, and our capacities are far inferior as compared to other warm blood mammals
of the animal kingdom. The whale and the polar bear have physical features that allow them to remain in freezing waters for
indefinite periods.
In 1967 Ted Erikson became the first swimmer to complete one of the coldest swims recorded. This was a 30 mile swim in
the Farallon Islands near Golden Gate Bridge in San Francisco in temperatures of 50-55F. Lynn Cox took the record for the l
ongest swim recorded in the coldest water conditions. In l987 at the age of 30 years she was able to tolerate, unharmed and
under close medical supervision a 2.5 mile swim that separates the Diomede Islands in the Arctic Ocean. The water temperature
was recorded around 44F (6-8 C) where she remained until completion for 2 hours and 6 minutes.
On December 13, 2003, at the age of 46 years Lynn Cox was able to swim 1500 meters in 22 minutes in the Antarctic Ocean in
36F water. Two days later she swam 1900 meters in 33 F water in 25 minutes. She recovered unharmed. Her body temperature
was measured at 35.2F when she stepped ashore and it normalized after one hour. She was accompanied by observers and
Emergency Room physicians. This feat was accomplished wearing only a bathing suit, cap and goggles. Her swim was recorded
and broadcasted on TV recently.
These cases are extraordinary and unusual. The average human tolerance is far below this. It is a commonly held belief that
an untrained person of 50 years has a 50% chance of surviving a 50 meters swim in 50F water in swimming trunks.
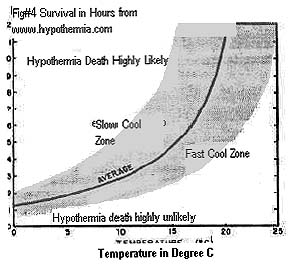 Figure #4 describes a tolerance curve to immersion in cold water. The graph compares length of immersion in hours vs.
water temperature plotting the likelihood of survival. The lower right side of the curve pertains to the rapid cooling people
and showing that the length of survival in 5-10C (42-50F) water is approximately one hour. This is the reason why rescuers
call the first hour "the crucial hour". All available efforts must be enlisted to rescue victims stranded in cold waters within that
window in order to obtain maximize survival. The gray part of the curve takes into account slow cooling people (to the left of
the curve) and fast cooling people who have a chance of surviving shorter periods. Nevertheless, even when immersed in water
up to 20C (68F) can result in fatalities within hours. The fatalities increase exponentially and dramatically after 12 hours
Figure #4 describes a tolerance curve to immersion in cold water. The graph compares length of immersion in hours vs.
water temperature plotting the likelihood of survival. The lower right side of the curve pertains to the rapid cooling people
and showing that the length of survival in 5-10C (42-50F) water is approximately one hour. This is the reason why rescuers
call the first hour "the crucial hour". All available efforts must be enlisted to rescue victims stranded in cold waters within that
window in order to obtain maximize survival. The gray part of the curve takes into account slow cooling people (to the left of
the curve) and fast cooling people who have a chance of surviving shorter periods. Nevertheless, even when immersed in water
up to 20C (68F) can result in fatalities within hours. The fatalities increase exponentially and dramatically after 12 hours
Surprisingly, even well conditioned, properly trained and experienced English Channel swimmers have suffered unexpected
fatalities within relatively short periods of 5-6 hours after the onset of their swim in water temperatures of 20C (68F).
Individual tolerance is highly variable and can be significantly diminished when conditions are poor such as cold ambient
temperature and rough weather conditions. Bad weather can lengthen the duration of the swims inducing extreme fatigue
and exposure. Prolonged swims in water temperatures below 16C (60F) particularly when the ambient temperatures are
low and in absence of sunny conditions could lower the resistance and tolerance of the individual swimmer and might explain
adverse outcomes.
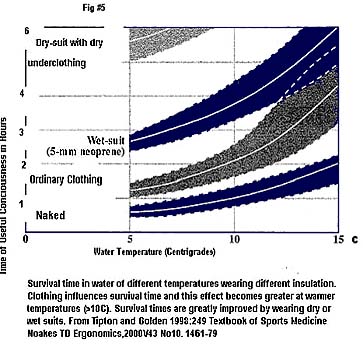
Figure #5 documents survival times in water of different temperatures when wearing clothing of different insulation. Note
that clothing influences survival times and that this effect becomes greater at warmer temperatures >10C (50F). The lower
curve is without clothes, the middle curve is with ordinary (street) clothes, the 3rd curve is with a wet suit, and the 4th is with
a dry suit and dry clothes.
When the temperature of a swimmer undertaking a long distance event, reaches 35C (95F), the first observable sign is a
serious (60-70%) reduction in their ability to perform mental tasks such as reasoning, memorization, repetition and calculations.
This useful practical information can help those monitoring them during long events in cold waters. This information helps the
trainer to determine if the swimmer's body temperature is nearing 34C (93F).
 There are currently sophisticated systems that allow monitoring by telemetry of body internal temperature. These systems
utilize pill size temperature diode transmitters from the person's gut by emitting vibrations. Continuous or intermittent readings
of the body temperature would be available. These systems are still somewhat expensive and slightly cumbersome.
There are currently sophisticated systems that allow monitoring by telemetry of body internal temperature. These systems
utilize pill size temperature diode transmitters from the person's gut by emitting vibrations. Continuous or intermittent readings
of the body temperature would be available. These systems are still somewhat expensive and slightly cumbersome.
They are still considered by most participants as an intrusion into the essence of the sport.
An athlete's ability to complete a long and demanding event in cold water, lasting many hours is highly dependent on the
integrity of their physiologic processes that allow the body to generate energy and therefore heat, as reflected in a steady
forward pace.
If respiratory problems develop as a result of bronchospasm from cold temperature or salt water ingestion, the oxygenation
of the blood may become inadequate depriving the muscle of the necessary substrates to renew sources of energy.
When the muscles are unable to obtain sufficient nutritional supply which is mainly glucose, because of inadequate or low supply
of at least 30-60gm/hour, the muscle begins to rely on the anaerobic sources producing increasing amounts of lactic acid, thus
speeding up fatigue and inability to sustain a prolonged effort. Other causes diminishing the glucose supply are poor absorption,
because of gastric intolerance (sea-sickness), or from prolonged vomiting due to intake of salt water or sea.
An inadequate absorption of fluids and nutritive factors may cause dehydration. Even minor dehydration will in turn diminish
the swimmer's capacity to generate work and heat. A vicious circle will develop leading inevitably to hypothermia within a
matter of minutes or hours.
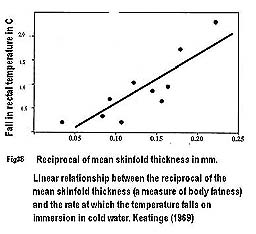
Figure #6 shows the linear relationship between the reciprocal of the mean skinfold thickness (a measure of body fatness)
and the rate at which the temperature falls on immersion in cold water. In other words, the thicker the skinfold the less the
body temperature falls. Specifically there is a linear relation in the fall of rectal temperature when immersed in 15C (59F)
cold water for 30 minutes. Increasing body fatness diminishes the rate of body cooling. Calculations have been made showing
that each 1mm increase in the thickness of the subcutaneous fat layer reduces the body cooling in cold water immersion by
raising the body's tolerance to the cold water by 1.5C. Lanolin and grease, when applied to the skin in amount of 1 mm
thickness, increases the fat layer by 1 mm and raises the perception and tolerance of cold water temperature by 1.5C (Pugh
et al 1960).
 Tipton in 1999 found that swimming in cold water at 10-18C (50-64F), increases heart rate, oxygen use, respiratory
frequency and inspiratory volume producing hyperventilation. He found that a decrease in swimming performance,
defined by a change in swimming efficiency, was closely correlated with the skinfold thickness of the upper limbs. He concluded
that the arms were particularly susceptible to cooling when swimming for prolonged periods in cold water and that a greater
subcutaneous layer around them, would promote more effective and prolonged function allowing greater stroke length and better
position in the water.
Tipton in 1999 found that swimming in cold water at 10-18C (50-64F), increases heart rate, oxygen use, respiratory
frequency and inspiratory volume producing hyperventilation. He found that a decrease in swimming performance,
defined by a change in swimming efficiency, was closely correlated with the skinfold thickness of the upper limbs. He concluded
that the arms were particularly susceptible to cooling when swimming for prolonged periods in cold water and that a greater
subcutaneous layer around them, would promote more effective and prolonged function allowing greater stroke length and better
position in the water.
Swimming in temperatures of 9-11C (49-51F) requires a great deal of adaptation. In this temperature range an individual
can quickly lose the capacity to interpret or detect a precipitous drop in their internal temperature, because cold perception
is severely altered by the development of limb anesthesia. A drop of the body temperature to 32C (89.6F) could be fatal when
accompanied by heart irregularities and ventricular fibrillation.
The observer should be attentive to a sudden change in posture of the swimmer's body. The development of hypoxia causes
the swimmer's stroke to shorten with an increase in the stroke rate or frequency. The swimmer's body will start sinking,
because of the adoption of a more vertical position. This will in turn lessen the efficiency of the swimmer causing slowing of
forward progress.
Drowning can occur in a hypothermic swimmer when muscular weakness impairs their ability to maintain open airways,
because of the development of laryngeal spasm or stoppage of breathing (respiratory apnea). This can occur in more advanced
stages of hypothermia.
The rescue, recovery, and survival are more seriously compromised in those hypothermic swimmers that have been
recovered after salt water has entered into their lungs.
GENERAL RECOMMENDATIONS FOR FIRST AID
TO A PERSON SUSPECTED OF HYPOTHERMIA:
- Determine if the person is hypothermic by palpating their chest or back (if not wet). If the person is wet register
internal body temperature (rectal or ear canal). Severe hypothermia is <30C (86F).
- Evaluate vital signs: BP, pulse respirations.
- Assess mental functions: language, orientation and speech; is the person's speech slurred? If so remove the person
from the water.
- If all the above is normal then it is most likely a mild hypothermia.
- After removing the person from exposure, cover them with blankets or in a large plastic trash bag, covering the
head with a hat, neck with scarf and gloves.
- Call emergency systems immediately for transport to medical facility.
- If there is warm water make warm water bottles and place them under the axillae (arm pits), and around the neck
(back of the head)
- If the person is alert, use a warm shower.
- Place the person in a sleeping bag with another person of normal body temperature (not hypothermic) to radiate heat.
- Administer warm fluids by mouth if alert, conscious and able to swallow.
- In absence, low or irregular pulse and respiration, commence CPR if there are no contraindications.
- Administer oxygen if available. Administer IV fluids during transport to medical facility.
BIBLIOGRAPHY:
1. Best CH, Taylor NB Physiologic basis of Medical Practice Williams and Wilkins 1961 7th Ed. Chap 52 Body
Temperature.
2. Hypothermia Publications State of Alaska, Cold Injuries, Water near drowning Publications and Protocols
www.hypothermia-ca.com 7/02.
3. Hypothermia Prevention, Recognition and Treatment. www.hypothermia.org.
4. Danzl, D.F., Pozos, R.S. Accidental Hypothermia New England Journal of Medicine 1994 :(226):1757.
5. Conrad Wennerberg. Wind Waves and Sunburn. A brief history of Marathon Swimming, 1997. Breakaway Books.
6. Noakes T.D. Exercise and Cold. Ergonomics, 2000, vol (43), No 10, 1461-79.
7. Keatinge W.R. 1969. Survival in Cold Water (Oxford, Blackwell Scientific).
8.Keatinge W.R., Khartchenko, M., Lando, N., Lioutov, V., Hypothermia during sport swimming in water below 11C.
British Sports Med: 2001, Oct, 35(5) 352-3.
9. Tipton M, Eglin C, Gennser, M., Golden, F. Immersion deaths and deterioration in swimming performance in cold water
volunteer trial. 1999 Lancet 354, 626-9
10.Acevedo EO, Meyers MC, Hayman, M. Haskin, J. Applying physiologic principles and assessment techniques to swimming
the English Channel. A case study. J. Sports Med Phys Fitness 1997, March 37(1)78-85
11. Pugh, L.G.C.E., Edholm, O.G., Fox,R.H.,Wolff, H.S.,Hervey, G.R.,Hammond, W.H., Tanner, G.M., and Whitehouse, R.H.,
1960, A physiological study of channel swimming, Clinical Science, 19,257-273.
12. SwimInfo. Lynn Cox Swims a Mile in Antarctic Ocean. Feat to Be Shown on 60 Minutes. February 6, 2003.
www.swiminfo.com
13.Lynne Cox. Swimming to Antarctica. Personal History. The New Yorker. February 3, 2003; pp: 66-74.